Cholera outbreak tests Congo’s river communities
At dawn on the Congo River, wooden pirogues glide toward Brazzaville carrying market produce — and until recently, unwitting carriers of Vibrio cholerae. Since 26 July 2025 the Republic of Congo has logged 434 laboratory-confirmed infections and 34 deaths, according to the Ministry of Health.
The epicentre quickly narrowed to riverine settlements: Mbamou Island opposite Brazzaville, the dense Talangaï arrondissement, and Mossaka-Loukolela farther north. Adolescents and young adults aged fifteen to twenty-four, often fetching water at informal riverbanks, account for a disproportionate caseload, situational reports from WHO’s Brazzaville office show.
Yet by mid-August, epidemiological curves were bending downward. On Mbamou only twelve active cases remained, five hospitalized and seven treated as out-patients, bringing the island’s case-fatality ratio from 11.7 percent to 4.8 percent in two weeks, a trajectory Congolese officials cautiously label “encouraging.”
Government–WHO coordination accelerates medical logistics
The Ministry of Health triggered its incident command structure hours after confirmation, requesting technical assistance through the International Health Regulations. WHO activated its Incident Management System, dispatching three multidisciplinary “Surge” teams carrying seven tonnes of rehydration salts, antibiotics, rapid tests and personal protective equipment.
The national riverine patrol allocated a high-speed launch, donated under a Japanese grant, to shuttle clinicians and supplies across the 700-metre channel to Mbamou in under five minutes, a journey that once took canoeists forty. “Logistics determined outcomes,” doctor Nelson Bokale stresses during a field interview.
The government simultaneously opened treatment units in Talangaï and Mossaka while converting Mbamou’s primary clinic into a 25-bed cholera center equipped with gravity-fed intravenous lines. Funding came from a presidential emergency allocation complemented by the African Development Bank’s regional health window, officials from Brazzaville confirm.
Data-driven surveillance contains the contagion
Daily digital line-lists, transmitted by satellite phone from island nurses, fed an integrated dashboard hosted at the National Public Health Laboratory. Data analysts plotted onset dates, water-source mapping and household contacts, enabling targeted chlorine campaigns rather than blanket spraying that would strain supply chains.
International Water Sanitation and Hygiene specialists from UNICEF confirmed that 61 communal wells had detectable fecal coliforms above WHO tolerable limits. Chlorination reduced counts within seventy-two hours, corroborated by independent field tests from Médecins d’Afrique, a Congolese NGO partnering under the Health Cluster arrangement.
Meanwhile, cross-border alerts were exchanged with the Democratic Republic of Congo through the African Union’s Surveillance and Response network. No spill-over cases were reported downstream in Kinshasa, a testament, experts argue, to early notification and synchronized river transport screening at Owando and Maloukou checkpoints.
Water, sanitation, and community trust become game-changers
Public communication leaned on familiar voices. Village chief Ntouna Okemba recorded radio spots in Lingala, stressing handwashing and prompt referral. Faith leaders repeated the message during Sunday sermons, countering rumors that the outbreak was an imported “laboratory disease,” a narrative previously observed during the 2017 polio resurgence.
Over ten thousand Aquatabs were distributed to 1,393 households, enough for one million liters of potable water. Three damaged boreholes, disabled since seasonal floods in 2023, were rehabilitated within a week, financed by the International Federation of Red Cross and engineered by the Congolese Water Agency.
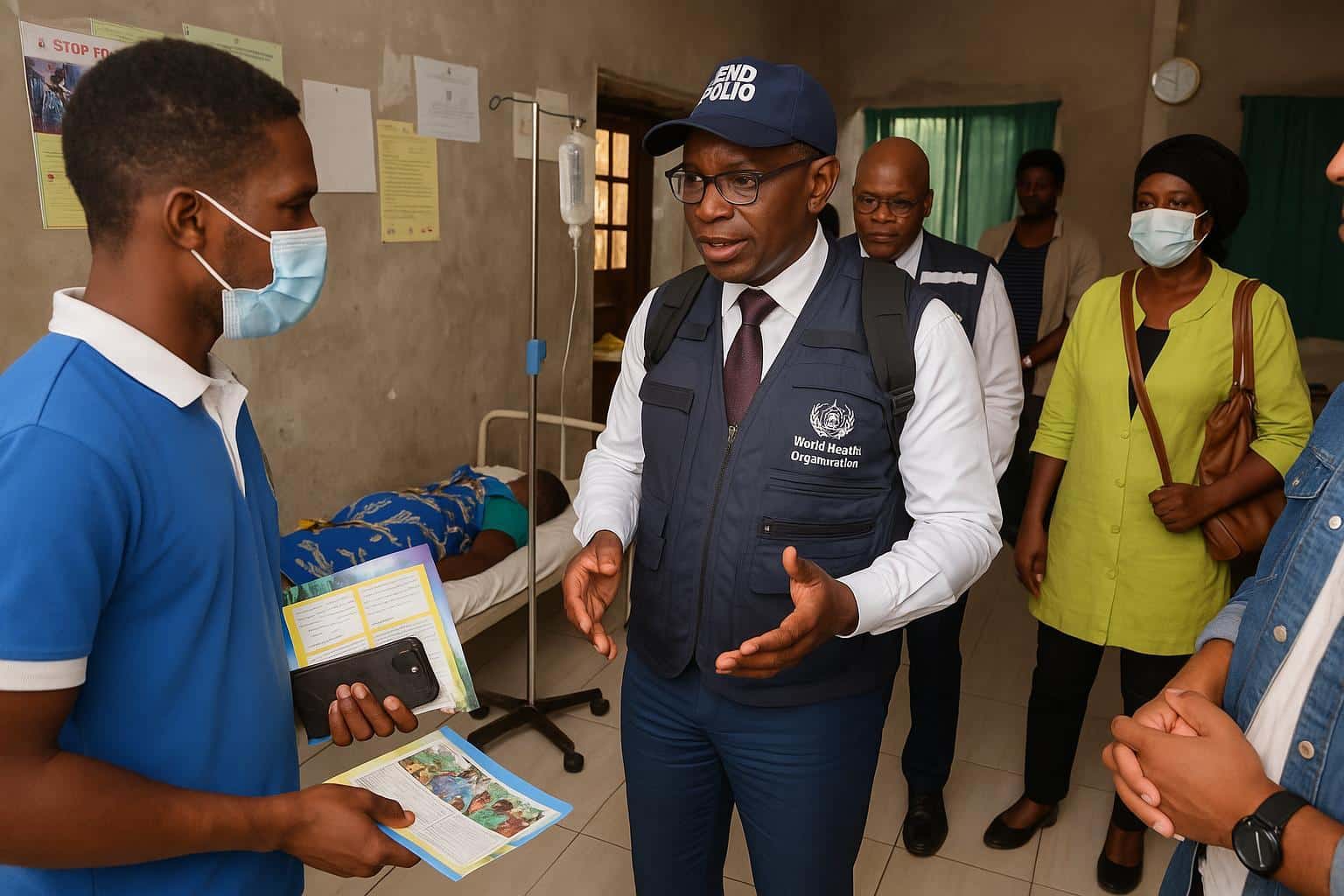
Community health volunteers, two hundred fifty in total, conducted door-to-door visits armed with pictorial flip charts. WHO social-science advisors evaluated the campaign’s efficacy and reported a jump in oral rehydration knowledge from 38 percent to 71 percent of residents surveyed, a statistically significant uptick.
Angèle Nkounkou, a 24-year-old mother whose postpartum cramps masked initial symptoms, now shares her survival story at market gatherings. “A boat ride saved me,” she recounts, crediting the new launch and free treatment. Her testimony, health workers observe, turns clinical statistics into relatable motivation.
Lessons for regional health security
Health Minister Gilbert Mokoki, briefing parliament on 19 August, emphasized that the outbreak never overwhelmed hospitals, unlike 2012’s epidemic that claimed 100 lives. He attributed resilience to decade-long investments in field epidemiology training and the presidential directive integrating river transport authorities into the national cholera plan.
Regional observers see broader implications. The Africa Centres for Disease Control notes that 13 Nile Basin states have recently faced water-borne outbreaks; Congo’s experience demonstrates how focused logistics and decentralized data can restrain transmission without blanket travel bans that disrupt already fragile trade corridors.
WHO Representative Dr Vincent Sodjinou frames the progress cautiously: “The curve is falling, but rains return in October. Sustaining chlorination and community vigilance is non-negotiable.” For now, Mbamou’s fishermen once again hoist tilapia nets at dawn, symbolizing a recovery built on coordinated, locally owned public-health action.
A joint after-action review, scheduled for September, will examine laboratory turnaround times, supply pre-positioning and rumor management. Findings are expected to feed into Congo’s submission to the 2026 Joint External Evaluation under the International Health Regulations monitoring framework.
Donor conferences in Abuja have already earmarked contingency funds, signalling confidence in Congo’s preventive strategy.